Building “Capacity” in the Baseball Pitcher
Let’s face it: Throwing a baseball at near-maximal velocities is inherently stressful. As such, pitching is not exactly an activity that lends itself well to being repeated hundreds of times each week over the course of a long competitive baseball season. Yet, that is exactly what baseball demands of its pitchers.
So, rather than rewrite the rules, it’s important that pitchers develop the ability to withstand and positively respond to the stresses they will experience — both in games and in practice — across the competitive season.
Why? Well, a pitcher who is not adequately prepared to handle the volume of throwing required of him in both training and in competition is at a much greater risk of suffering a catastrophic injury.
This is not a new concept.
Sports medicine professionals have long acknowledged the potential dangers of throwing too much and too frequently, particularly in youth baseball players, whose bodies lack the physical maturity of their adult counterparts.
With the rising trend of Tommy John surgery (see the figure from Liu et al. below), efforts are being made at both the amateur and professional levels of baseball to reduce the risk of overuse injury by restricting total throwing volume.
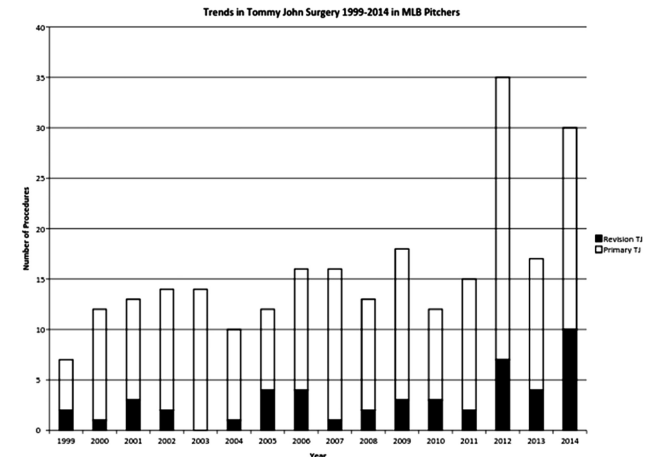
Tommy John surgery is on the rise. (Figure from Liu et al., 2016.)
For instance, Major League Baseball’s PitchSmart guidelines for youth and adolescent pitchers involves strict pitch counts (based on chronological age), in addition to ensuring adequate rest between pitching appearances. Although it’s far from perfect, this initiative is a good starting point for reducing the likelihood of young baseball players pitching in a fatigued state.
Many of the injury reduction strategies at the professional level are based on the same concepts of rest, pitch counts, and often poorly designed (or implemented) physical longevity programs.
What’s interesting to us at the BPG, is that all of these injury prevention strategies are focused on reducing demand — that is, the physiological and psychological load experienced by the athlete during sport — by modifying variables that are external to our pitchers.
As we discussed in our recently-launched webinar, we feel that the baseball world at large places too much emphasis on reducing the physical demands of competition (i.e. throwing volume) at the expense of efforts to better prepare our pitchers (in training) to withstand and even prosper under those same demands.
Don’t get us wrong: Matching demand to each pitcher’s level of physical preparedness is undoubtedly important for reducing the risk of overuse injury. But, it’s only one side of the injury (prevention) equation. So what’s the other side?
Demand Vs. Capacity
Injury prevention resides in the ability of the athlete to withstand the demands of competition — something we like to call capacity. As such, the injury prevention equation is characterized by the intricate balance between capacity and demand.
Demand >> Capacity = Injury
Demand > Capacity = Adaptation
Capacity > Demand = Prevention
When the demand placed on the athlete is much greater than his capacity, the risk of injury goes up substantially. A perfect example of this is the young professional pitcher who doubles his innings pitched in his first year with the Big Club and lands himself on the disabled list.
However, when the right amount of demand is appropriately matched to an athlete’s current abilities — i.e. when there’s less of a “gap” between the athlete’s current abilities and what is being asked of him — the athlete will positively adapt to that new demand, and capacity improves.
Improve an athlete’s capacity to the point that it exceeds the demands of competition, and you’ve got yourself an equation for injury prevention.
Aside from directly improving performance, this is, in a nutshell, what most progressive strength and conditioning programs are designed to accomplish: Improve an athlete’s ability to withstand the demands of his sport, by exposing his muscles, tendons, joints, and nervous system to increasing loads/stressors over time.
But where many baseball strength and conditioning programs fall short is that they see improved capacity as simply a product of increased strength and/or muscle cross-sectional area, failing to acknowledge the full spectrum of physical and mental qualities that collectively make up an athlete’s overall or “comprehensive” capacity.
Capacity: It’s Not Only About Strength
Although the injury prevention equation seems simple at first glance, the term “capacity” is often misunderstood, or poorly defined. It is commonplace for coaches to associate capacity with an athlete’s ability to withstand Newtonian force. In the case of pitching, this is reduced down to: how much cumulative torque load can a pitcher’s shoulder or elbow withstand within a given time period?
It’s a good start, but it’s a bit narrow-minded; it doesn’t constitute a wide enough spectrum of analysis. That is, for injury prevention, we need to be concerned with more than just strength.
For example, it is often cited that the flexor-pronator mass plays a significant role in protecting the ulnar collateral ligament (UCL) by dynamically stabilizing the elbow during valgus loading in the pitching delivery (e.g., Park & Ahmed, 2004). However, these conclusions are founded on evidence from studies of human cadavers, which makes it hard to draw conclusions about living subjects, let alone overhead throwing athletes.
Still, these studies have led some strength and conditioning coaches and sports medicine specialists to the conclusion that to reduce injury to the UCL, pitchers must simply “strengthening the flexor-pronator mass”. Whether it’s wrist curls or elbow flexion exercises, or more specific modalities such as throwing weighted baseballs, every coach has their own methods for strengthening the flexor-pronator mass.
Some of these approaches do in fact hold merit for improving tissue capacity, a necessary component of “overall” or “comprehensive” capacity, but we believe that simply strengthening the flexor-pronator mass is an incomplete approach for reducing the risk of UCL injury. (If you’re interested why we believe this to be the case, check out our (free) webinar on Dynamic Systems and Motor Variability in Baseball.)
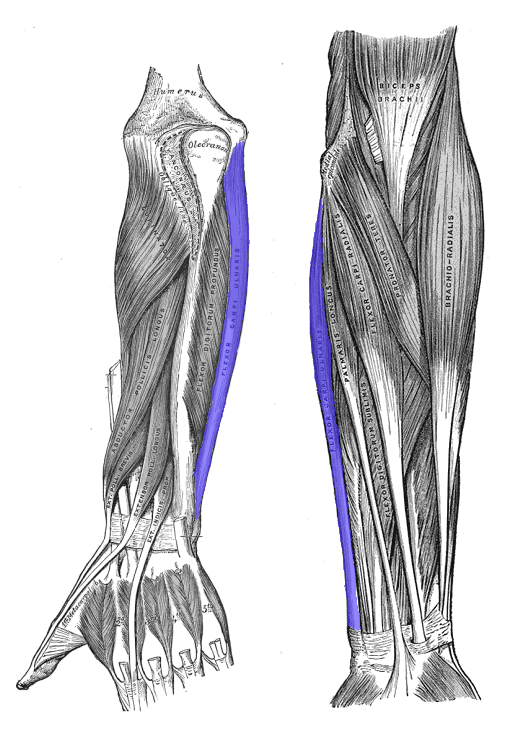
Strengthening the flexor-pronator mass is probably not the solution to the Tommy John epidemic.
Even if improving the capacity of the muscular tissue that “shields” the UCL was the most significant factor — it’s still an incomplete approach to developing comprehensive capacity. To adequately prepare our pitchers for competition, we need to explore other (equally important) avenues. Building capacity requires a multimodal, comprehensive approach, in which improving tissue capacity is only one.
That being said, the importance of tissue capacity cannot be understated, and is elegantly summarized by physiotherapist and tendon scientist Professor Jill Cook:
“Your tissue capacity will only ever be as great as the load you place on it.” ~ Professor Jill Cook
The practical significance of tissue capacity for physical preparation, is that tissues need to be trained (progressively) to be able to withstand the loads they will experience during sport. In the case of pitching, this might refer to the capacity of the tissues of the shoulder and elbow to withstand external rotation and valgus torque, respectively*.
*These are just examples. The shoulder and elbow experience a diversity of forces throughout the throwing motion.
But, importantly, when we’re talking about tissue capacity, we’re not justtalking about the structural and functional characteristics of muscle. Connective tissue responds to load too. And when we’re talking about connective tissue we’re not just talking about tendons — all connective tissue responds to load, whether that connective tissue is tendon, ligament, articular cartilage, or bone (to name a few). This occurs via a process calledmechanostransduction:
“[…] the process by which the body converts mechanical loading into cellular responses. These cellular responses, in turn, promote structural change.”(Khan & Scott, 2009).
Although the process of mechanotransduction is rather complex, the concept is relatively straightforward. Most of us are familiar with Wolff’s Law (bone will remodel itself over time to to accommodate increased loading) and there is clear evidence that exercise can promote denser trabecular networks and greater cortical thickness in bone (Haapasalo, 2000).
The same general principle holds true for other connective tissue as well. For instance, the tendon literature clearly shows that net collagen synthesis in tendon increases in response to physical training, thereby increasing tendon stiffness and physical robustness (Langberg, Rosendal and Kjaer 2001).
Other fibroblastic derivatives such as ligaments, cartilage, joint capsules, and fascia also seem to be mechanosensitive and thus can all improve their capacity to withstand load. Even if the changes are as minute as altering the laying down of collagen in a parallel over a haphazard fashion, that would still lead to an increase in tissue capacity! (It is beyond the scope of this article to go into more detail on this subject, but we will be releasing an article specifically on connective tissue capacity soon.)
In the case of preventing something like Tommy John surgery, the implications of mechanotransduction are substantial: ligaments such as the ulnar collateral ligament can (and should!) be the target of therapeutic approaches just as much as muscular tissue such as the flexor-pronator mass.
Movement Capacity
“You’re always going to regret not training the position you got hurt in.” ~ Dr. Andreo Spina
Movement capacity is, very simply, the ability to perform and better tolerate a wide range of movements. Here, we are referring not only to the ability to passively access a large amount of articular range of motion (i.e. passive range of motion), but also the ability to actively control it.
There is a common misconception that flexibility in and of itself is a desired trait. But, in our eyes, range without control is a useless commodity (most of the time). What we are really looking for is “mobility”, what we define as the ability to actively move in and out of various ranges of motion.
This requires a particular attention to detail. As we have mentioned in previous articles (see here and here), we want our pitchers to be able to demonstratearticular dissociation — the ability to independently control one joint without including another.
For example, if we are assessing or addressing internal rotation of the glenohumeral joint, we want to appreciate whether or not the scapula comes along for the ride. As noted in our webinar, the importance of this dissociation between adjacent joints is critical to the self-organization process. (You can read more about self-organization and pitching here.) By improving controlled articular range, we are providing the central nervous system with a much richer sensory landscape, which it can then use to better configure the appropriate (or necessary) coordination pattern.
This makes intuitive sense: A pitcher with good hip, spine, and shoulder mobility is going to have a much greater number of movement “solutions” at his disposal compared to a pitcher who doesn’t move as well.
The functional role of this motor variability for reducing the risk of overuse injury cannot be understated. Namely, the greater the coordinative variability between individual biomechanical degrees of freedom within the movement system, the greater the ability that system has to offset the load at any one particular joint, such as the elbow, and, instead, distribute that load more evenly throughout all of the involved biomechanical degrees of freedom.
Physiological Work Capacity
Generally speaking, work capacity refers to an athlete’s ability to perform his sport at a high level of performance for an extended duration of time, both in training and competition. Note that work capacity is specific to the demands of the sport. (This is important.)
For a pitcher, work capacity refers to the ability to maintain both velocity and command from pitch-to-pitch over the course of an inning, and from inning-to-inning over the course of a game; it involves both the general aerobic capacity as well as the specific local muscular endurance (or is it more appropriate to say speed-endurance?) required to throw a baseball up to 100+ times a game.
Importantly, general aerobic capacity is just that: general. Want to be able to throw more and for longer? Throw. But that doesn’t mean that general aerobic conditioning won’t benefit pitchers either.

Pitching deep into ball games is the most tried and true way to get better pitching deep into ball games. But that doesn’t mean we can’t develop the appropriate energy systems through more general means as well.
Despite the reliance on anaerobic alactic (or ATP-PC) energy system during the execution of a single pitch, the aerobic system is absolutely vital for improving the energy system pathways that replenish the ATP-PC systembetween pitches (and between innings).
Furthermore, low-intensity aerobic conditioning work will improve the pitcher’s general work capacity — the ability of the heart, lungs, and vascular system to deliver oxygen to the working muscles and remove metabolic “waste” — which will allow him not only to go deeper into ballgames but also to do more work in practice/training. (Which is key if he expects to get better over time.) Plus, you can’t discount the implications of aerobic exercise for overall health!
Psychological Capacity
Up until this point we have talked mainly about capacity in terms of biological tissue, physiology and movement complexity, but it would be a huge mistake to not address the most under-looked aspect of them all: psychological capacity.
We loosely define psychological capacity as:
“the ability to maintain rapt attention and intention towards the task, and appropriate arousal levels, given the dynamic in-game conditions and emotions that afflict the athlete during competition.”
That is, when the game throws us a proverbial curveball, and things don’t go our way — or maybe when they are really going our way — how well do we maintain our mental composure?
The importance of the mental game is talked about all the time. (And for good reason!) The deleterious effects of anxiety and pressure have been demonstrated time and time again in the literature. Rob Gray, a research professor out of Arizona State University, showed that in simulated high pressure situations, golfers showed more internally directed focus of attention, reduced movement variability, and overall poorer performance. In fact, under these high pressure scenarios, elite golfers reverted to movements consistent with those of novices! (Gray, 2013.)
At the BPG, we believe part of our goal as coaches should be to build up the psychological capacity of our athletes to withstand the negative effects of cognitively- and emotionally-challenging scenarios. To achieve this optimal psychological state, we must develop the ability to control our arousal levels and direct our intentions towards the task at hand.
This psychological state in which optimal performance occurs is what the famous psychologist Mihaly Csikzentmihalyi termed the “Flow State”. His definition elegantly describes a state in which most of us have felt at the pinnacle of our game:
“[…] being so involved in an activity that nothing else seems to matter. The ego falls away. Time flies. Every action, movement and thought follows inevitably from the previous one. Your whole being is involved, and you’re using your skills to the utmost.” (Csikzentmihalyi, 1990.)
Mentally, our goal is to tap into this state as much as possible. Attaining flow, puts us into a state of hypofrontanality — it shuts off the overly analytical part of our brain. Our implicit system — the action system — takes over and our decision making is fluid, in the moment, and automatic. We are placed in a state where awareness and action meet simultaneously; we get out of the way of ourselves and “just do it”. Dietrich described this as “taking the brakes off”, trading energy reserved for higher thinking and problem solving for awareness and attention.
At the BPG, it is our belief that attaining a flow state reduces the internal (organismic) constraints on the movement system, such as anxiety and/or internally-directed focus of attention. Flow allows the pitcher’s implicit system to work freely, opening up room for variability in the coordination of his pitching delivery via self-organization.
Flow: The Psychology of Optimal Experience. A must read for coaches.
It should be obvious that we should be chasing this flow state as much as possible, but at the same time we must acknowledge that flow is indeed a rare event. Having said that, hypofrontanility is a state that can be more easily achieved the more that we are exposed to it, and can be driven by other forms of practice like meditation, mindfulness and visualization. At the BPG, we believe that achieving flow is absolutely necessary for optimal performance
Another crucially important, but seldom discussed component of psychological capacity is something probably best referred to as, “pain literacy”. Sports medicine is still largely based on biomedical paradigms, and attempts to integrate modern pain science with traditional explanations of mechanical pain in sports injury are still in their infancy.
The acknowledgement of neurobiological, psychological, and sociocultural influences on mechanical pain is (for the most part) completely lacking in the sporting world (baseball is no exception) yet these biopsychosocial influences have major implications for performance and rehabilitation.
For instance, an athlete’s perception of pain (i.e. what pain means to them) may influence to what degree pain affects their motor strategy in training and competition (Hodges & Moseley, 2003). A pitcher who perceives elbow pain to be indicative of tissue damage may exhibit less movement variability (as a protective strategy) than a pitcher who understands that “hurt” does not necessarily equal “harm”. (We briefly discussed the difference between pain and injury here.)

R.A. Dickey’s transition from college flamethrower to Major League knuckleballer is an extreme example of what perceived threat (even in the absence of pain!) can do to your pitching delivery.
In this sense, the perceived threat of throwing a baseball in a pitcher with a history of arm pain constrains the pitching delivery much in the same way performance anxiety does. As such, changing our athletes’ perceptions about pain is something we foresee as being absolutely necessary for improving psychological capacity, injury resiliency, and ultimately optimal performance.
In fact, we believe that improving pain literacy could prove to be just as fruitful for injury prevention as tissue capacity, work capacity, or movement capacity. Most importantly, it is the development of all “types” of capacity — that is,comprehensive capacity — that will help reduce the incidence of throwing injuries in baseball.
Major Takeaways
- For injury prevention, we cannot focus solely on reducing demand. Rather, we need to begin shifting more attention to building overall capacity.
- Capacity is a commonly misunderstood term in the baseball community, and is not limited to the structural and functional characteristics of muscle alone. Comprehensive capacity consists of many different “types” of capacity including tissue capacity, movement capacity, physiological capacity, andpsychological capacity.
- A comprehensive injury reduction strategy will requires an individualized approach to improving each of these types of capacity, which collectively will improve resiliency: the system’s overall ability to withstand demand.
References
- Park, M. C., & Ahmad, C. S. (2004). Dynamic contributions of the flexor-pronator mass to elbow valgus stability. J Bone Joint Surg Am, 86(10), 2268-2274. https://www.ncbi.nlm.nih.gov/pubmed/15466738
- Khan, K. M., & Scott, A. (2009). Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. British Journal of Sports Medicine, 43(4), 247-252. https://bjsm.bmj.com/content/43/4/247.short
- Haapasalo, H., Kontulainen, S., Sievänen, H., Kannus, P., Järvinen, M., & Vuori, I. (2000). Exercise-induced bone gain is due to enlargement in bone size without a change in volumetric bone density: a peripheral quantitative computed tomography study of the upper arms of male tennis players.Bone, 27(3), 351-357.https://www.ncbi.nlm.nih.gov/pubmed/10962345
- Langberg, H., Rosendal, L., & Kjær, M. (2001). Training‐induced changes in peritendinous type I collagen turnover determined by microdialysis in humans. The journal of physiology, 534(1), 297-302.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2278680/
- Gray, R., Allsop, J., & Williams, S. E. (2013). Changes in putting kinematics associated with choking and excelling under pressure. International Journal of Sport Psychology, 44(4), 387-407.
- Csikszentmihalyi, Mihaly (1990). Flow: The Psychology of Optimal Experience. New York: Harper and Row. ISBN 0-06-092043-2
- Hodges, P. W., & Moseley, G. L. (2003). Pain and motor control of the lumbopelvic region: Effect and possible mechanisms. Journal of Electromyography and Kinesiology, 13(4), 361-370.https://www.ncbi.nlm.nih.gov/pubmed/12832166
baseballdevelopmentgroup.com
baseballdevelopmentgroup.com
Kirk Herring
Lonnie Bishop
Lien Corral
Joanna Le Souef
Spencer Beuzeville